Results of CWCI Survey on Telemedicine/Other Claim Administration Changes
Last week the Institute surveyed our members to gather industry input on some of the changes that are being proposed to the med-legal process, as well as other challenges of delivering benefits and administering claims during the COVID-19 crisis. We wanted to gauge how ready and willing claims organizations are to leverage telemedicine for QME evaluations and other services.
The Institute would like to thank everyone who responded to the survey on short notice. Many of the comments received provided valuable insight on where and when telemedicine could be viable, as well as issues that will need to be addressed to implement this type of change. We will be sharing the de-identified results of the survey with the DWC Administrative Director who asked us to gather the opinions, suggestions, and comments from our members on these potential changes.
Each of the questions from the survey, along with the results and comments received for that question, are summarized in the following pages.
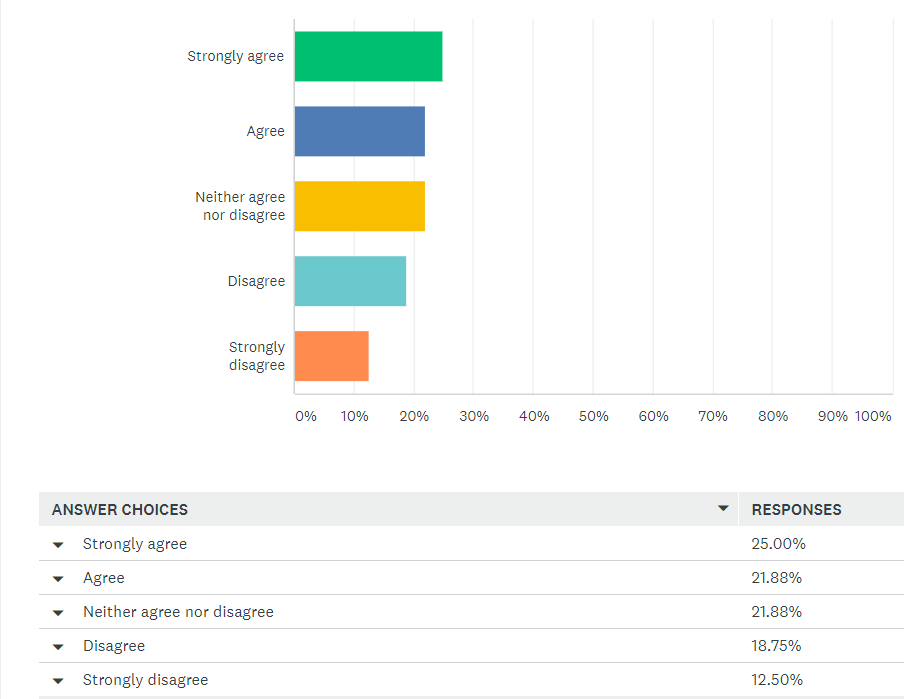
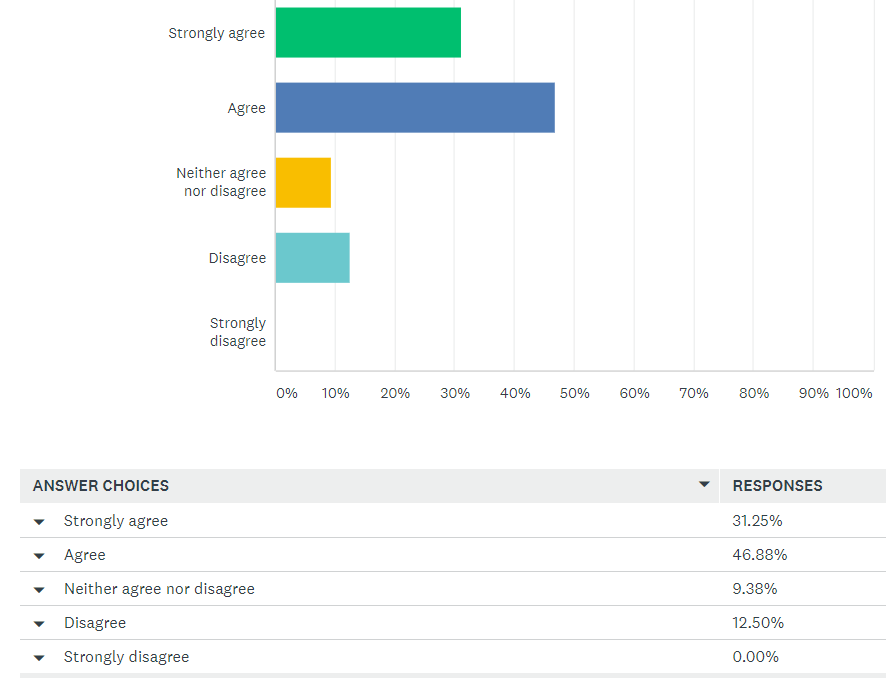
Question 1: Your organization is able to provide injured workers with basic resources to be able to participate in a telemedicine evaluation from their home (e.g., sending a link to download and install an app on the claimant’s smartphone).
Comments:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
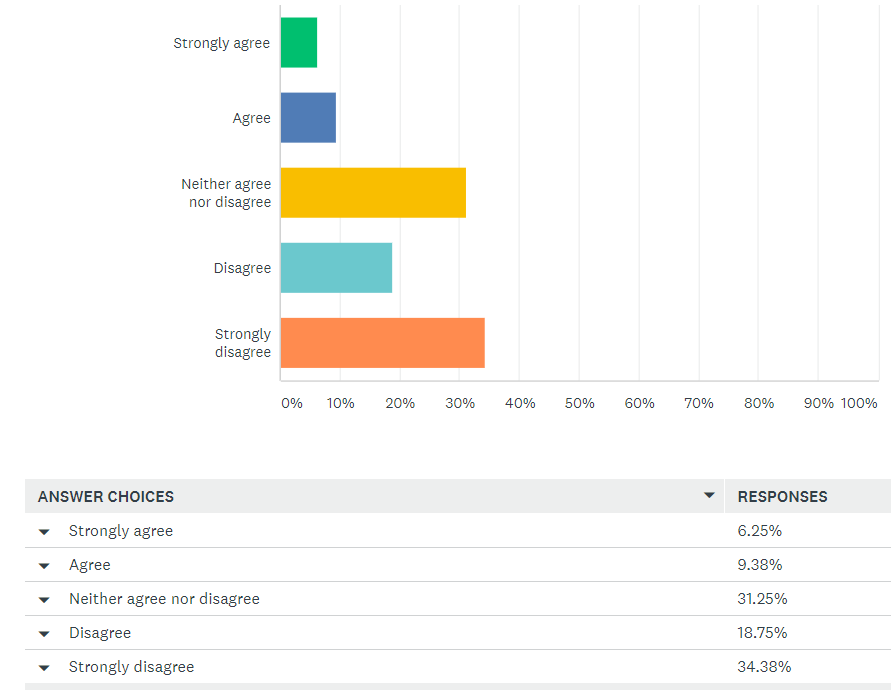
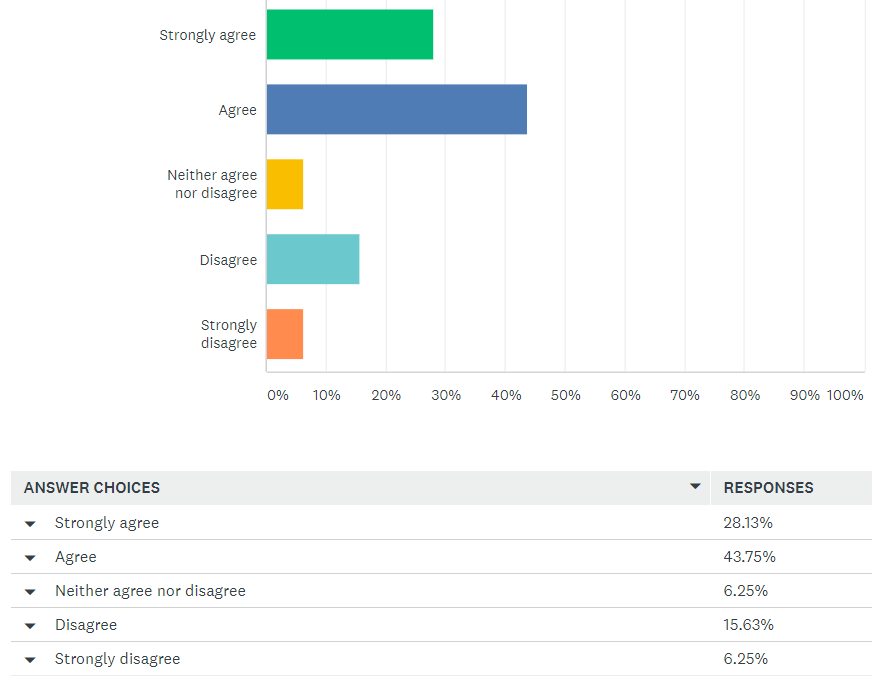
Question 2: Your organization is able to provide injured workers with more expansive resources to be able to participate in a telemedicine evaluation from their home (e.g., delivery of a monitoring or diagnostic device to the claimant’s home, with instructions).
Comments:
|
|
|
|
|
|
|
|
|
|
Question 3: In what situation(s) would your organization consider consenting to the use of telemedicine in the med-legal realm?
Comments:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Question 4. In what situation(s) would your organization never consider consenting to the use of telemedicine in the med-legal realm?
Comments:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
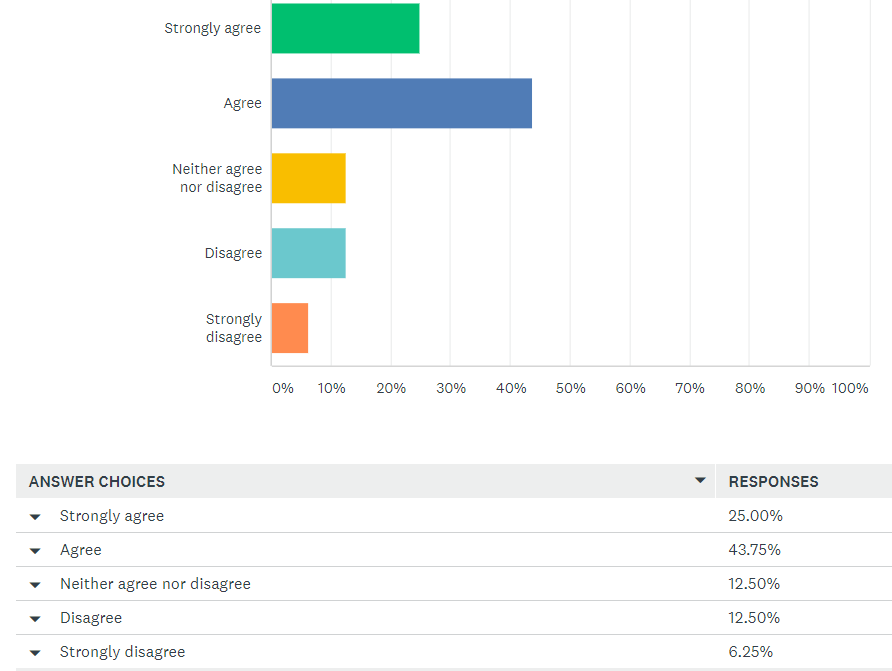
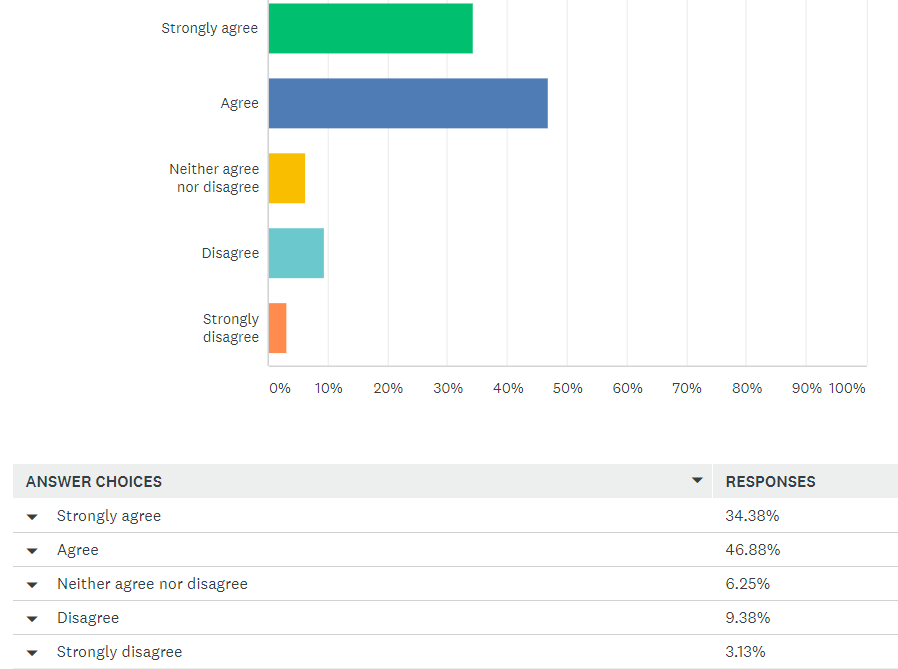
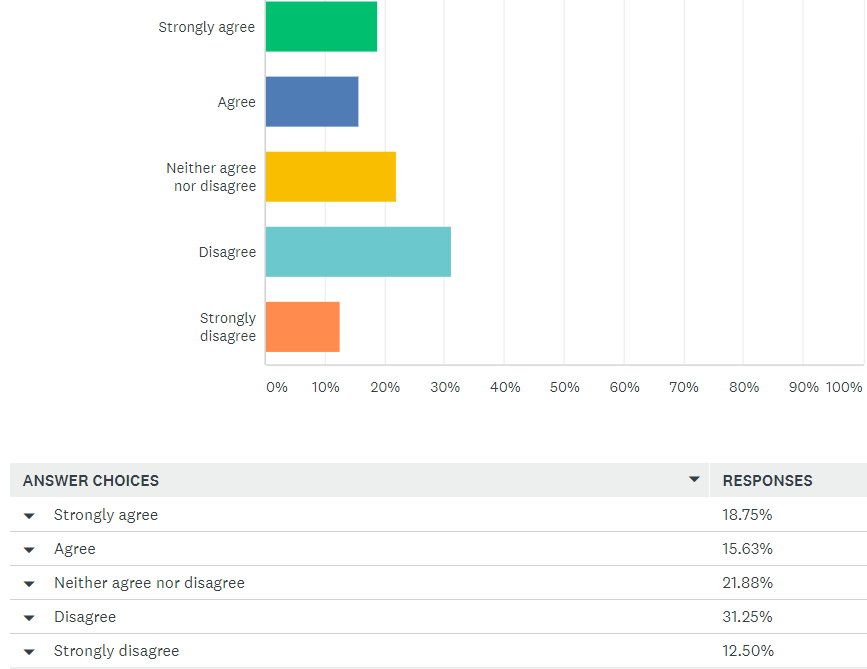
Question 5: During the present COVID-19 crisis, the DWC Medical Unit should permit remote telemedicine evaluations instead of in-person examinations per §4062.1 and/or §4062.2 in order to avoid appointment cancellations, delays in reporting, and interruption of the med-legal process.
Comments:
|
|
|
|
|
|
|
|
|
|
|
|
|
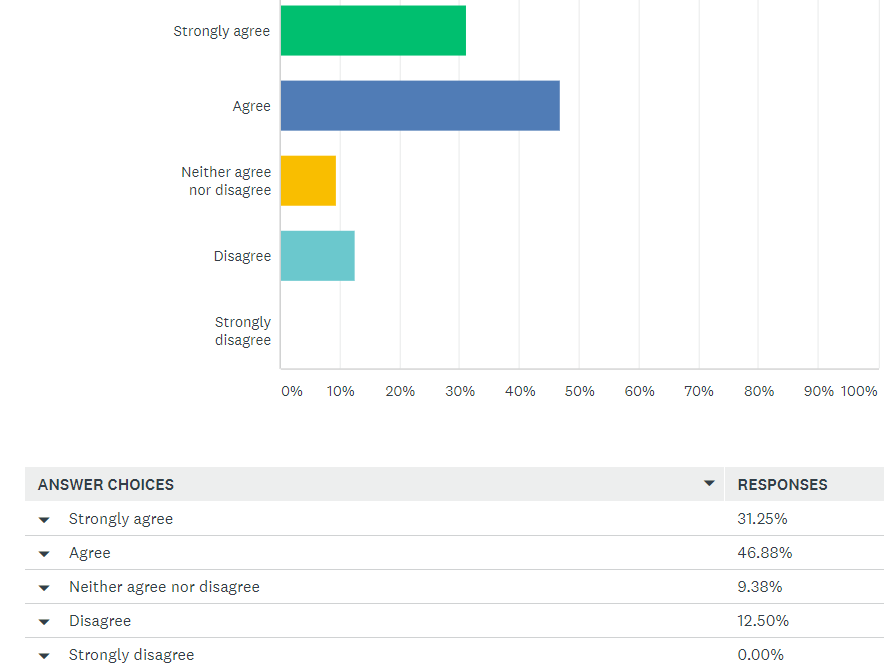
Question 6: The timeframe for an Agreed Panel QME or QME who cancels an evaluation to reschedule the appointment per 8 CCR §34(e) should be extended to a date within 60 calendar days of the cancellation and not more than 90 days from the original request for an appointment (i.e., a 30-day extension of this regulation), unless the parties agree to a longer period.
Comments:
|
|
|
|
|
|
|
Question 7: An AME evaluator who cancels an evaluation shall reschedule the appointment per 8 CCR §34(f) within 90 days of the cancellation, unless the parties agree to a date no more than 30 calendar days beyond the 90-day limit (i.e., a 30-day extension of this regulation).
Comments:
|
|
|
|
|
|
Question 8: The 60/90-day timeframes for the requesting party to obtain a QME appointment per 8 CCR §31.3(e) should be replaced by 90/120-day timeframes (i.e., a 30-day extension of this regulation).
Comments:
|
|
|
|
|
|
|
|
Question 9: The requirement that the initial QME evaluation take place at the location listed on the Panel Request form should be waived.
Comments:
|
|
|
|
|
|
|
|
|
Question 10: The 30/60-day timeframes for the med-legal physician to issue initial/supplemental reports per 8 CCR §38 should be replaced by 90/120-day timeframes (i.e., a 30-day extension of this regulation).
Comments:
|
|
|
|
|
|
|
Question 11. Do you have any suggestions or issues concerning questions of AME/QME reimbursement?
Comments:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
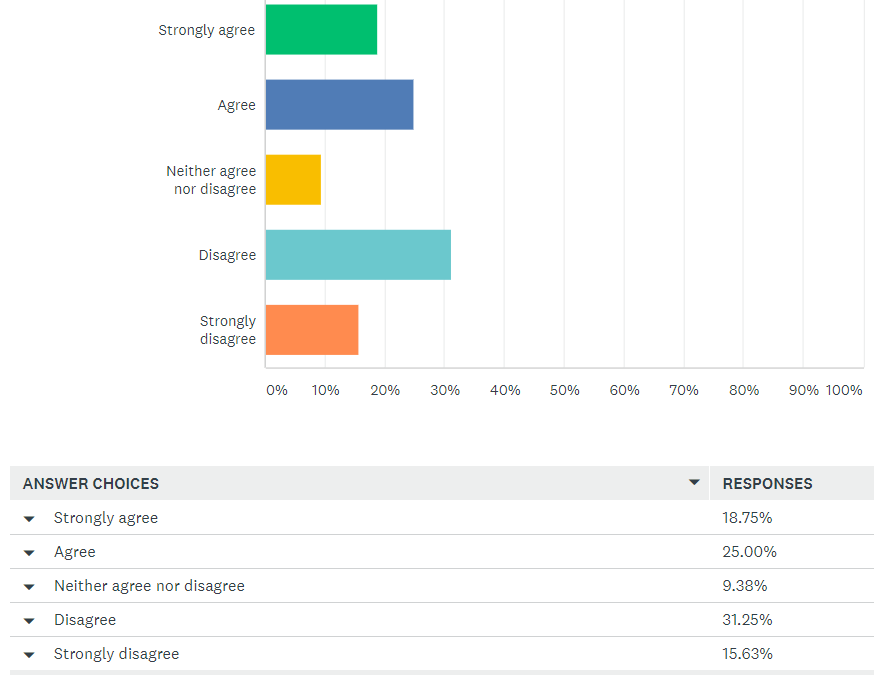
Question 12: The current health crisis and Shelter-in-Place directive have disrupted your organization’s ability to meet statutory deadlines for delay/denial letters, benefit notices, Explanations of Review, etc.
Comments:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Question 13: Please use this box to raise other urgent concerns outside of QME-related issues.
Comments:
|
|
|
|
|
|
|
|
BY/